
A controversial approval of an Alzheimer’s treatment reveals a core weakness in oversight of agency discretion.
Alzheimer’s disease is an irreversible, progressive brain disorder that slowly destroys memory, cognitive skills, and, eventually, the ability to carry out simple tasks. Alzheimer’s disease—ranked as one of the top six leading causes of death in the United States—has long evaded scientists’ and researchers’ efforts to find an effective treatment.
On June 7, the U.S. Food and Drug Administration (FDA) approved aducanumab, a therapy for the treatment of Alzheimer’s disease sponsored by Biogen, which will be commercialized under the brand name Aduhelm. Aduhelm was the first treatment for Alzheimer’s approved by FDA since 2003. Its approval has generated widespread controversy and concern rather than celebration, as public health experts question both the validity of the approval process and the benefits of the drug.
Although much of the current debate is focused on the unique features of this particular drug and the consequences of its approval, we suggest that the approval can be best understood within a more general framework that increasingly characterizes FDA decision-making, which we define as “regulatory reactivity.” Regulatory reactivity is a shift in agency decision-making processes that appears compliant with legal frameworks and long-held regulatory postures while at the same time departing from regulatory standards. Understanding Aduhelm’s approval as the result of regulatory reactivity can help isolate areas of regulatory weakness and support targeted institutional reforms.
The approval of Aduhelm by FDA was noteworthy for at least three reasons. First, pharmaceutical companies have invested significant resources in developing treatments for Alzheimer’s disease for over two decades, but virtually all of them have failed to receive FDA approval on grounds of insufficient safety and efficacy. Aduhelm seems to suffer from the same shortcomings as many other nonapproved treatments.
Second, Aduhelm was approved using an “accelerated approval pathway,” which allows FDA to approve drugs for serious conditions that fill an unmet medical need, even if the drug was not shown to have a direct therapeutic effect on the disease itself. Under the accelerated approval pathway, the drug sponsor need only show that the drug affects a “surrogate” clinical endpoint. This endpoint could be a laboratory measurement, radiographic image, physical sign, or some other measurable unit that is thought to reasonably predict—but is not itself a measure of—clinical benefit. In cancer drugs, for example, tumor shrinkage may be used as a surrogate clinical endpoint for the clinical benefit of increasing cancer patients’ survival.
In the case of Aduhelm, FDA approved the drug based on a surrogate clinical endpoint of decreasing levels of a protein called amyloid-beta, which accumulates in the brain of Alzheimer patients and is considered a possible cause of loss of nerve cells, a characteristic of the disease. Clinical trials of Aduhelm, however, have not conclusively shown that it improves the condition of Alzheimer’s patients; they only show that Aduhelm decreases the levels of amyloid-beta clumps—known as amyloid plaques—in Alzheimer patients’ brains.
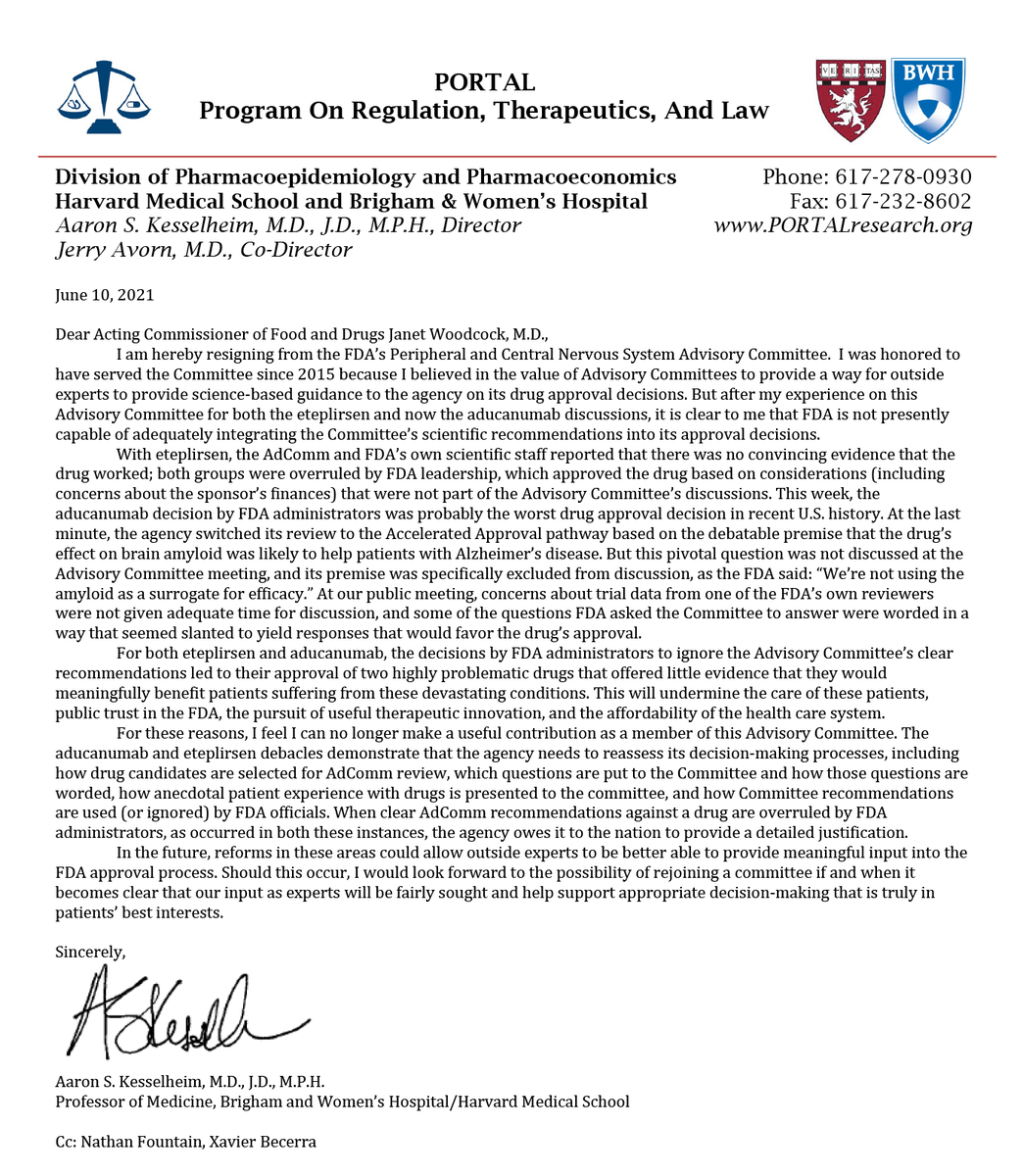
Third, and most unusual, was the approval of Aduhelm despite the explicit and near-unanimous recommendation of FDA’s own Peripheral and Central Nervous System Drugs Advisory Committee against approving aducanumab for the treatment of Alzheimer’s without further testing.
Within the first week following the approval, three out of eleven members of FDA’s Advisory Committee resigned in protest. One of the resigning members reportedly branded the evaluation and approval of Aduhelm a “sham process,” and “foreordained,” and another resigning member gave it the dubious title of “probably the worst drug approval decision in recent U.S. history.” These comments depart from the usually polite and restrained discourse of FDA Advisory Committees.
The resigning members of the Advisory Committee cited many reasons for their resignations. All of their reasons involve concerns with the evaluation and approval process for Aduhelm, including the following:
- FDA’s decision to approve Aduhelm despite a lack of evidence that the drug was effective in reducing Alzheimer’s symptoms while having evidence of significant adverse reactions;
- The last-minute switching of Aduhelm from the regular approval track to the accelerated approval track without consultation with the advisory committee, which effectively sidestepped the advisory committee’s recommendation not to approve the drug;
- The reported presentation of “biased questions” by FDA’s review staff when asking the advisory committee to evaluate Aduhelm;
- Denying the recommendation to require further clinical testing by Scott Emerson—an FDA statistician who reportedly likened FDA’s presentation of information to the advisory committee to the Texas sharpshooter fallacy in its framing; and
- FDA approval of the drug “based on considerations … that were not part of the advisory committee discussions,” including FDA staff concern for the drug developer’s finances.
Independent advocacy groups and experts—who have expressed strong opposition to the approval of Aduhelm ever since its clinical trial results came out in 2020—echoed these concerns. In the wake of FDA’s approval, these groups decried the agency’s decision as not rooted in science and as potentially harmful to public health.
Critics have raised concerns about how closely Biogen worked with FDA during the approval process, pointing to “unusual” features of the collaboration and the level of influence that industry-funded patient advocacy groups may have on FDA.
Approval against the recommendation of an advisory committee is not unique but is very unusual. A study published in 2019 found that between the years 2008-2015, FDA only deviated from advisory committee recommendations in about 22 percent of cases in which an advisory committee opinion was sought. Of these 22 percent, FDA chose to adopt a less restrictive position than the Committee’s recommendations in only about 1 in 4 cases. Historically, then, FDA has decided to adopt a more lenient course of action than its advisory committees’ recommendations in about 5 percent of cases. But approving a drug against the near-unanimous disapproval of an advisory committee is almost unprecedented.
The controversial approval process for Aduhelm is symptomatic of a more significant problem with the decision-making framework at FDA. As Sam Gandy, a professor at Icahn School of Medicine at Mount Sinai put it, “decisions that ought to be science-based are being increasingly driven by politics, wishful thinking, and even delusion.”
In a forthcoming article, we develop the concept of “regulatory reactivity” to reflect agency decisions that, while seemingly consistent with applicable legal frameworks, in practice constitute a worrisome departure from evidence-based standards.
Regulatory reactivity has several hallmarks: non-adherence to predetermined principles, standards, and operative procedures in reaching an agency decision; direct reaction to pressure, whether internal or external, political or non-political; and results that further short-term agendas rather than long-term goals.
Regulatory reactivity occurs when extraneous pressures lead an agency to set aside its own procedures, expertise, and priorities—frequently under the guise of regulatory nimbleness—to reach a preordained result, often in pursuit of short-term goals. When operating in “reactive mode,” for example, FDA may use the flexibility afforded by an expedited pathway to issue an authorization or approval that is not supported by the available data and guiding principles. Currently, no mechanisms in administrative law effectively check regulatory reactivity.
The approval of Aduhelm meets the criteria of regulatory reactivity. FDA ignored scientific evidence and experts’ opinions, possibly as a result of outside pressure—by patient groups and, in different ways, by the drug makers. They did so while setting aside their own standard approval procedures to attain what appears to have been a predetermined, short-term outcome designed to respond to a burning and elusive public-health need. In so doing, FDA undermines the raison d’etre of having expert agencies in the first place, while also damaging public trust and the agency’s already-battered reputation.
In the context of health-oriented agencies such as FDA, regulatory reactivity is problematic because it unmoors agency decisions from their consequences for public health, aligning decisions with special interests rather than with health outcomes. Such decisions fail to capture the actual costs, risks, and benefits—or lack thereof—of a given marketing authorization or approval. They may also result in potentially detrimental effects on public health and—as observed during the COVID-19 pandemic—decrease public trust in the agency’s decision-making processes.
In the case of Aduhelm, if further trials prove the drug to be ineffective in treating Alzheimer’s disease, then the approval is expected to result in significant harm to Alzheimer’s patients and an enormous waste of funds used to meet Aduhelm’s price tag of $56,000 a year.
Regulatory reactivity not only provides a lens to examine a breakdown in decision-making, but also calls attention to a breakdown in regulatory oversight. Regulatory reactivity falls within a gray zone of agency decision-making that may escape judicial review. Existing judicial review frameworks allow agencies broad discretion in fashioning responses to problems. When operating in reactivity mode, agency decisions and actions lack evidentiary support, reliability, accountability, and fairness, and they are prone to conflicts of interest. Yet reactive decisions generally do not rise to the level that would prompt a court to set them aside, particularly when agency decision-making requires balancing competing interests while considering a complex subject matter in which the agency exercises expertise. Since the agency can provide seemingly credible justifications for adopting a given measure through the selective use of reasoning that meets current legal standards of administrative law, it is difficult to show that such justifications mask interests, agendas, or goals that the agency should not be pursuing. The departure from the agency goals is, thus, difficult to challenge and rectify.
One possible way of curbing regulatory reactivity would be to tighten statutory requirements that bind agencies to evidence-based decision-making. Such requirements would seek to limit outside pressure by tethering agencies to predetermined standards and procedures, making it harder to change course without clear, evidence-based justifications.
Changing the standards for evaluating agency actions by courts is another way to address reactivity. Courts have been highly deferential to agency decisions and actions within an agency’s statutory purview, as called for under the Chevron doctrine.
The scope of the Chevron test makes it ill-suited to address reactivity problems. By nature, reactivity problems derive from facial compliance with an unambiguous statutory or regulatory framework. This facial compliance masks the true roots of the problem: an unambiguous framework used as a shield to justify reactive behavior that is substantively inconsistent with the agency’s mission. So, the traditional checks offered by the Chevron framework are of little help to reactivity problems.
Another possible way of decreasing regulatory reactivity within the Chevron framework would be for courts to employ a diminished level of Chevron deference when agencies act in ways that go against expert advice or scientific understanding of the issue at hand but are nonetheless justified by reasoning that evades characterization of the decision as “arbitrary or capricious.” In the event of such a departure from the recommendations of scientific experts, the court would no longer be required to follow step two of the Chevron test but would instead apply a non-deferential standard of review.
Both of these proposals are likely to be controversial, and both would require significant changes to current law. As a more modest interim measure, we have, in an earlier essay argued for the establishment of an independent, binding review mechanism for FDA’s decisions to increase public trust in the agency’s decisions surrounding the approval of treatments for COVID-19. Such a measure, although cumbersome, could curb FDA reactivity. FDA’s recent decision to approve Aduhelm constitutes an additional example of why such an independent external review deserves serious consideration. The current controversy over Aduhelm may serve as a window of opportunity for garnering support for such a change.





{kind=link}